Presbyopinion

Part II: Management options
Everyone has an opinion on presbyopia. But let’s stick to the facts and answer this question: What is presbyopia, exactly, and what can we do about it? Using an evidence-based approach with information from recently published review papers, this article explores the ins and outs of presbyopia and its correction methods based on the British Contact Lens Association’s (BCLA) Continued Learning Evidence-based Academic Report (CLEAR) on presbyopia, comprising more than 175 pages distributed over eight peer-reviewed articles.
Part I here in GlobalCONTACT covered the mechanism of accommodation and presbyopia as well as definitions of the condition. This part focuses on management options as an alternative to glasses. Contact lenses are certainly included, but the CLEAR papers are not limited to that option; intraocular lenses (IOLs), corneal surgical techniques, pharmaceutical solutions and even scleral technology will be discussed.
Presbyopia manager
Eye care practitioners, especially those in optical outlets, most often focus on glasses first as an option for presbyopia. Often, the term ‘presbyopia’ is replaced by ‘you need reading glasses’ when practitioners speak to patients. This unnecessarily limits patients’ management options. The current generation of emerging presbyopes is the first generation that grew up with contact lenses as a default correction in high school, rather than glasses. That generation is eagerly searching for a way to correct their reading issues without glasses. Contact lenses and IOLs seem to be the big ‘go to’ options for that group, maybe along with some corneal, pharmaceutical and new scleral techniques. Here is an overview.
IOLs
The first IOLs were introduced shortly after World War II, not by coincidence (because of cockpit canopies made of polymethylmethacrylate [PMMA]). But it was not until the 1980s that IOLs were used to correct presbyopia (monovision in 1984, multifocal [MF] in 1987). Two major developments assisted this innovation: the invention of phaco-emulsification techniques that permitted much smaller incisions, and the use of foldable intraocular lenses. This often results in non-stitch surgeries with very limited invasion of the cornea and anterior ocular surface.
There are many IOLs available (over 100 lens designs are mentioned in the paper, but there are probably many more in parts of Asia). It is interesting though, that only a small portion of cataract surgeries are done with multifocal IOL designs. In essence, there are three main types of MF IOL options: in addtion to spherical lenses for monovision, concentric/extended depth of focus (EDOF) designs and trifocal lenses. All lenses other than those with a spherical optical design are typically considered ‘premium’ (MF designs in addition to toric lenses). EDOF designs can be a good option for patients working primarily at an intermediate distance (e.g., computer screen). Trifocal lenses are designed to offer good distance and near vision while also trying to correct intermediate distance; their disadvantage can be a general loss of contrast sensitivity.
The big question with IOLs for presbyopia correction is: What is the condition of the crystalline lens? If there is any form of clinically significant cataract, the option to remove the crystalline lens and replace it with a MF lens design (or monovision) of some sort is often pretty straightforward. ‘Clear lens extraction’ is a different consideration. Many patients do not understand the implications of IOL implantation (giving up any form of rest-accommodation). It is important to clearly discuss this with the patient prior to the procedure. Any form of dry eye should be treated before undergoing the procedure, as the symptoms may worsen or may surface with IOL implantation.
If the optical outcome is not 100% satisfactory after IOL implantation, a ‘simple’ corneal refractive procedure (see next part) can be performed to correct any form of ametropia and/or astigmatism that is left over. Lens extraction (removing the lens) if the outcome is not satisfactory is possible but rare.
Experiments into accommodative lenses are gaining much attention in the research and development field but have not been hugely successful so far. Still, such a lens would be ‘the holy grail’ for presbyopia management going forward. In general, the relative popularity of IOLs for the correction of presbyopia shows that a large portion of the population wants an alternative to the conventional ‘reading glasses’ to optimize their near vision performance.
Creative with cornea
One of the CLEAR papers (#6) is fully dedicated to corneal techniques—although in reality, this is not considered one of the primary methods, but these options do belong in this overview. Laser-assisted in-situ keratomileusis (LASIK) and photo-refractive keratectomy (PRK) first come to mind within this category, but obviously these are primarily used for distance correction (e.g., myopia and to a lesser extend hyperopia). Of course, if you are already a hyperope, correcting that can help tremendously in the early stages of presbyopia to improve reading. But it is crucial to inform patients in general that around when they hit the age of 45, they will not be able to read anymore despite their laser surgery, as presbyopia has a different mechanism involving not eye length but diminishing flexibility of the crystalline lens as discussed in part I.
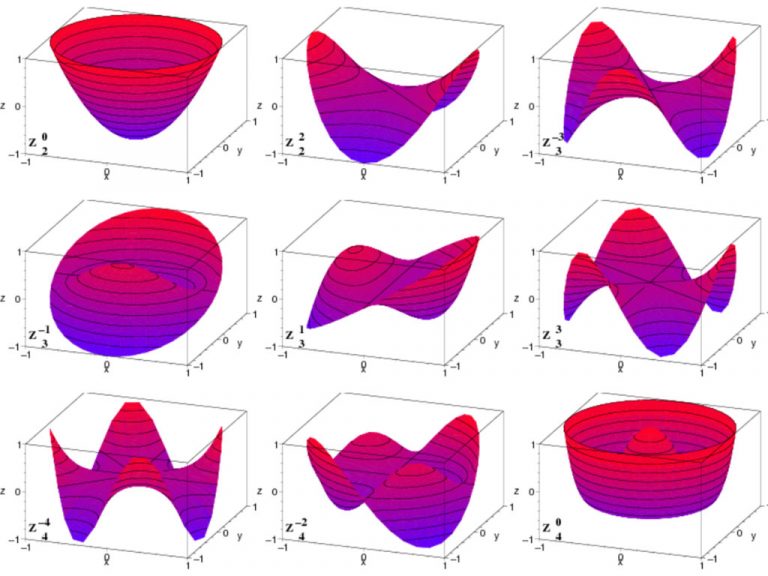
Alterations to the standard laser techniques for distance can be used to induce a spherical aberration profile in the cornea to support accommodation. Bi-aspheric MF ablation techniques create a prolate corneal shape, and the controlled induction of negative spherical aberration combined with induction of a low amount of myopia increases depth of focus.
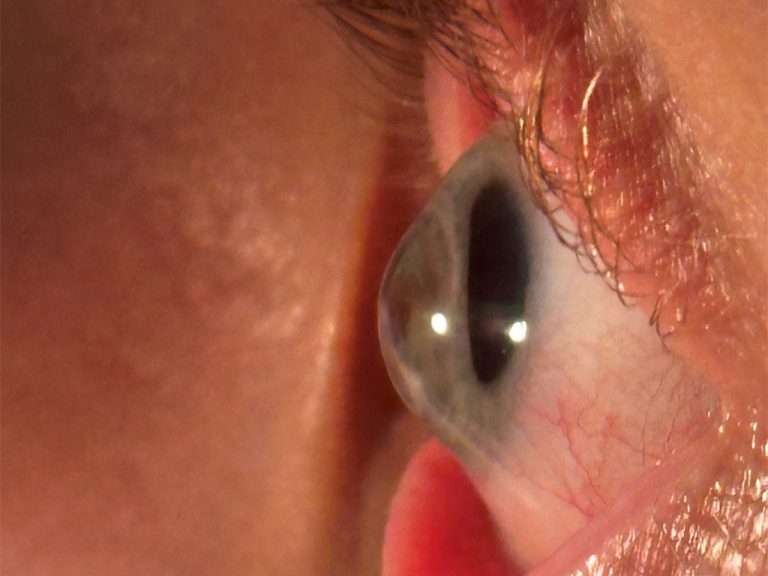
More experimental in nature are corneal inlays. Synthetic corneal inlays are made from artificial materials, such as acrylic, hydrogel or silicone. These inlays are designed to improve near vision by changing how light enters the eye, helping the eye focus on close-up objects. In essence, they use small-aperture optics to increase the patient’s depth of field without changing refractive lens power. These inserts are placed at various depths in the corneal stroma to improve near vision. The first corneal inlay received FDA approval in 2015. Using inlays with small openings effectively blocks the bending of light rays, minimizing refraction and improving near vision.
Conductive keratoplasty is mentioned here for the sake of the overview, but it is not a very commonly applied technique. Radiofrequency energy (350–400 kHz) is applied to the mid-peripheral corneal stroma, resulting in mid-peripheral corneal shrinkage and central corneal steepening that corrects hyperopia between +0.75D to +3.00D in theory.
As a general remark regarding corneal laser techniques: if IOLs are needed later in life, calculation of the lens power can be troublesome because the optics of the eye have changed. Corneal curvature and power values from before the procedure can be very helpful, and precise documentation of this by the ECPs is important. One main risk with many of the corneal techniques mentioned is dry eye symptoms; but as stated, this can be an issue with IOL implants as well.
Orthokeratology (ortho-k) in the CLEAR paper is regarded as an option under this category of corneal alterations – although the big difference of course is that ortho-k is less invasive, non-surgical and reversable. Although hard evidence is lacking, there are anecdotal reports indicating that the optics that ortho-k applies to the cornea centrally and peripherally can postpone presbyopia to some degree in the early stages.

Scleral crosslinking & more
The sclera has been a hot topic in the specialty lens field lately, but for an entirely different reason (e.g., scleral lens fitting). In reference to presbyopia papers (CLEAR paper #7), the issue is not so much the sclera’s shape but its rigidity. Aging makes the sclera more rigid, and a stiffer sclera ‘pulls’ more on the ciliary zonulae and muscles, which makes it harder for the crystalline lens to curve upon accommodation. To solve this, laser scleral microporation, in which the sclera is made more flexible, is proposed. The good news with this technique of course is that both the cornea and the crystalline lens are left intact. An interesting, but right now only an experimental and theoretical option.
The CLEAR paper also covers pharmaceutical intervention: in essence, pilocarpine. Different concentrations have been proposed in the past: 1%, 2% and 4%. Currently, a new US Food and Drug Administration (FDA) formula with 1.25% is on the market in the US. Pilocarpine produces a ‘simple’ pinhole effect, just like with the corneal inlays, as discussed.
Contact lenses
What do the CLEAR papers say about contact lens options for presbyopia, based on the latest evidence-based insights? According to the paper (#5 in the series), there are 101 contact lens designs for presbyopia. Granted, many of those are rigid lens designs, as there is simply more possible with that modality. In fact, in terms of vision & optics, rigid lens designs may be ‘world champions’ for presbyopic contact lens options, but 80% to 90% of lens fits (depending on region) in the world are with soft lenses. For the sake of time and space, let’s focus on soft lens options here.
Interestingly, if you boil it down, there are a few main MF optical categories – although there are many variables within the themes. And all of them (commercially available) are simultaneous lens designs, a term that is a bit misleading; it is not two images that are in focus simultaneously, but rather one sharply focused image superimposed over a blurry image. Depending on the direction of gaze and focal point, the brain chooses the image that it perceives as sharp(er). Within that group, concentric lens designs are the number one option. And almost all in the disposable soft contact lens group are center-near designs, meaning the near vision correction is in the center. Here, things start to diverge: the basic design has one ring of ‘distance power’ surrounding the near center, others have an extra ‘intermediate ring’ as a transition zone. Again, other alternatives are available with multiple rings for near and distance (but the central portion still contains the near addition). A variation is a center-near portion with a gradual (aspherical) optical transition to the distance power (not to be confused with the aspheric back-surface designs of some lenses to conform to the shape of the ocular surface).
The described EDOF design is a relatively ‘new kid on the block’ (a patent for this was granted in 2000). As with IOLs, this design literally increases the depth of focus of the lens by manipulating the higher-order aberration pattern, which makes them great for intermediate distances. Although EDOF designs may be a bit less dependent on lens centration, this is a problem with all simultaneous lens designs. Large pupils also can cause disturbances in vision due to an overlap of optical zone(s) within the pupillary zone. In theory, translating designs can overcome this, but they are only commercially available in rigid lens designs. Monovision is simple and cost-effective and is not pupil dependent, but it causes a reduction or loss in stereopsis and may only work well in low near-addition corrections (up to 1.5D typically).
In summary, the CLEAR papers are clear about a couple of things when it comes to MF soft lenses. There is no ‘one-size-fits-all’ solution for all patients. Concentric and EDOF designs (and individual options within those groups) all have their own unique advantages and challenges. Multifocal lens designs outperform monovision performance-wise, and daily disposable lenses can have benefits for patients (in terms of dry eyes and comfort). On the other hand, customization (in terms of lens shape, and optical design) can provide great benefits when correcting presbyopia – especially if in the future higher-order aberrations can be utilized, which will not be available as daily disposable options. Toric multifocal daily disposables, for instance, are not available yet; they may come soon, but with limited parameters at first is the expectation. Correcting astigmatism in presbyopes is one of the key tips for practitioners. As is ‘lose your pride, follow the guide’: lens manufacturers have spent millions of dollars developing their MF lenses, and they usually know better how to fit their lenses, but ECPs sometimes are a bit stubborn in this regard.
In closing
The increasing availability of different types of MF lenses, the expansion of parameter ranges, the improvements in optical designs, and the availability of customized lenses all offer great opportunities to satisfactorily manage presbyopia for a large segment of customers that desire them.
Eef van der Worp, BOptom, PhD, FAAO, FIACLE, FBCLA, FSLS is an educator and researcher. He received his optometry degree from the Hogeschool van Utrecht in the Netherlands (NL) and has served as a head of the contact lens department at the school for over eight years. He received his PhD from the University of Maastricht (NL) in 2008. He is a fellow of the AAO, IACLE, BCLA and the SLS. He is currently adjunct Professor at the University of Montreal University College of Optometry (CA) and adjunct assistant Professor at Pacific University College of Optometry (Oregon, USA). He lectures extensively worldwide and is a guest lecturer at a number of Universities in the US and Europe.
References:
- Craig JP, Barsam A, Chen C, Chukwuemeka O Jr, Ghorbani-Mojarrad N, Kretz F, Michaud L, Moore J, Pelosini L, Turnbull AMJ, Vincent SJ, Wang MTM, Ziaei M, Wolffsohn JS. BCLA CLEAR Presbyopia: Management with corneal techniques. Cont Lens Anterior Eye. 2024 Aug;47(4):102190.
- Morgan PB, Efron N, Papas E, Barnett M, Carnt N, Dutta D, Hepworth A, Little JA, Nagra M, Pult H, Schweizer H, Shen Lee B, Subbaraman LN, Sulley A, Thompson A, Webster A, Markoulli M. BCLA CLEAR Presbyopia: Management with contact lenses and spectacles. Cont Lens Anterior Eye. 2024 Aug;47(4):102158.
- Naroo SA, Woods CA, Gil-Cazorla R, Ang RE, Collazos M, Eperjesi F, Guillon M, Hipsley A, Jackson MA, Price ER, Wolffsohn JS. BCLA CLEAR presbyopia: Management with scleral techniques, lens softening, pharmaceutical and nutritional therapies. Cont Lens Anterior Eye. 2024 Aug;47(4):102191.
- Schnider C, Yuen L, Rampat R, Zhu D, Dhallu S, Trinh T, Gurnani B, Abdelmaksoud A, Bhogal-Bhamra G, Wolffsohn JS, Naroo SA. BCLA CLEAR presbyopia: Management with intraocular lenses. Cont Lens Anterior Eye. 2024 Aug;47(4):102253.