DEEP thoughts on soft lens fitting

Soft lens myths debunked
What an incredible vibe at the Global Specialty Lens Symposium (GSLS) 2026 at Paris in Las Vegas earlier this year. The energy and enthusiasm were truly of a higher order, with a strong focus on the application of higher-order aberrations in specialty lenses – going well beyond correction alone.
The meeting itself was outstanding: 850+ participants from more than 30 countries, 44 speakers, 34 continuing-education creditable hours, 140 posters, and 20 free paper and rapid-fire presentations, plus more than 60 participating exhibitors on the floor. A truly global and dynamic exchange of knowledge.
Keynote
One of the highlights for sure was the keynote lecture presented by Craig Norman and Patrick Caroline – the founders of GSLS – on the history of the meeting. It was interesting to see all that has happened in our industry since the first meeting in 2002 in Toronto, back when it was still the Global Orthokeratology Symposium. Myopia control had not kicked in; that did not surface until 2005 with important lectures by Brien Holden and Earl Smith at that year’s meeting. The meeting then transitioned to the Global Keratoconus Symposium in 2007, then later merged into all ‘specialty lenses’ together. Of course, the re-introduction of scleral lenses around the year 2010 was a major event that rocked the profession and the field to its core, which still resonates.
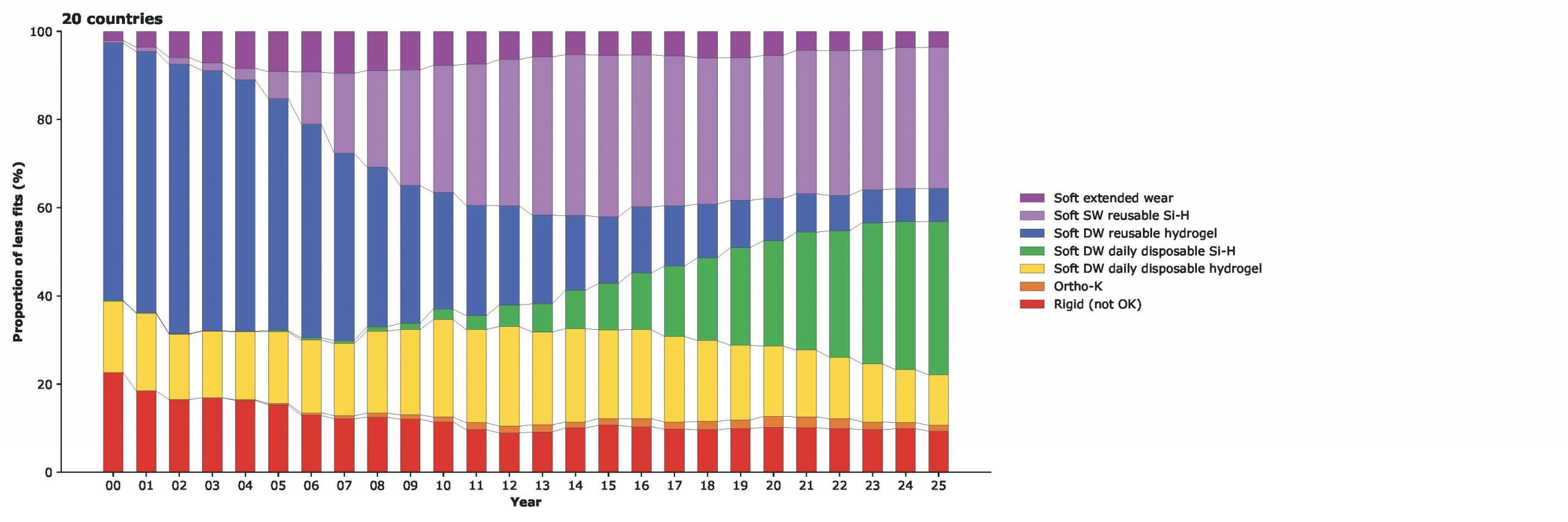
The titles of these meetings, and hence the bulk of the topics, of course, focus on ‘rigid’ lenses: ortho-k, corneal lenses, and sclerals, also at this year’s GSLS meeting. Interestingly, though, the vast majority of lens fits in the world are with soft lenses. According to the most recent Eurolens research data by Phil Morgan and colleagues from Manchester (UK), about 12% of fits are with rigid lenses (all types, the red and orange in the graph shown); hence, 88% of fits are with soft lenses worldwide.
The micron wave
When we focus on contact lens fitting among all these modalities, one thing becomes clear: it is all elevation based these days. In a recent article* in Contact Lens Spectrum, Randy Kojima, Matthew Lampa, and I dove into this, about how the whole industry is moving from base curves (in millimeters) to height data (in microns) with any type of lens, really. We have gotten very familiar and acquainted with this for scleral lenses, for ortho-k, and for corneal lenses too (the lathe ‘thinks’ in height, of course). Now the time seems right to embrace this approach for soft lens fitting as well.
Soft lens fitting?
If we focus on soft lens fitting, let’s first take a good look at the terminology. Are we fitting soft lenses or prescribing soft lenses? In reality, it is mostly the latter: the first myth about soft lens fitting is that we still fit them. We select a proven lens, based on our own clinical experience, or based on literature coverage or sometimes secondary considerations.
The thing is, we have better soft lenses now than we’ve ever had. The materials have improved tremendously over the years, and in terms of oxygen transmissibility and surface treatments, we have reached a point that not too long ago we could only have dreamed of. The biggest gain may be the frequency of replacement, though, up to daily replacement. Recent studies have shown that replacing lenses more often than once daily does not add much, at least not in terms of comfort or wearing success. The only thing you might add if patients start replacing lenses at midday (at work or school in suboptimal hygienic environments) is germs. Replacing lenses daily seems to be optimal.
Delving into dropouts
So that’s the good news. The bad news is that the soft lens dropout rate (the amount of lens wearers that start with soft lenses but discontinue) has not dropped in the last decade or so, as reported previously in this journal, too. The dropout issue is very complex, with the tear film, dry eye, and physiological processes involved. We have no control or influence over many of these aspects, though. What we do have some influence over as eye care practitioners is the lens fit. In an attempt to ‘tackle’ this inconvenient issue of dropouts – a problem for the entire international contact lens-industry – it would be nice to have a better way to assess our soft lens fits on-eye. This may be the biggest myth of all: that eye care practitioners have a solid or reliable way to accurately review soft lens fits behind a slit lamp. We unfortunately have limited ability to successfully assess a soft lens’ behavior on-eye.
Flat-fitting lenses are not usually the problem. A lens that has inadequate sagittal depth (is too flat) simply moves too much. We can see this behind the slit lamp quite easily; lens movement is excessive (in primary gaze while blinking or with the push-up test), the lens starts to decenter (usually in the temporal and/or inferior direction by the nature of the sclera’s shape) either slightly or excessively as the lens edge reached the limbal area. Also, lens wearing comfort is typically reduced, and vision can be compromised because of the decentration and/or movement (especially with more complex optics such as torics, multifocals, etc.). Here, we can do our job as eye care practitioners using the biomicroscope.
Going deep
Deep-fitting lenses, on the other hand, are a challenge. A recent experiment we performed at Pacific University in Oregon (US) showed that the differences between a good-fitting lens, a deep-fitting lens, and a very deep-fitting lens are hardly detectible. We fitted one eye with four different lathe-cut lenses with base curves of 7.7 mm, 8.0 mm, 8.3 mm, and 8.6 mm. Or, if you prefer, with sagittal depths of 4330, 4050, 3810, and 3610 microns, respectively. We used lissamine green dye for visibility purposes. The eye in question was a ‘normal eye’ with an average sagittal depth (SAG). The delta-SAG values (the differences between the sagittal depths of the lenses and the eye) were respectively 680, 480, 248, and 46 microns for the four lenses. A team of six very experienced contact lens experts in the field reviewed (blinded) the videos of these lenses on-eye – and could not find significant differences between the lenses; they assessed all four lenses as ‘acceptable for dispensing.’ Mind you, there was a difference in delta-SAG of about 650 microns among these four lenses.
On-eye diameter
Circling back to GSLS 2026, one lecture focused on a potentially better way to assess soft lens fits on-eye: by looking at on-eye diameter increase. Previous reports in this journal have indicated that if a deeper soft lens is placed on the eye, which is the default, the forces involved to ‘flex’ and to conform to the shape of the ocular surface need to go somewhere. Again, from a terminology standpoint, let’s stay away from ‘steep’ lenses and instead use ‘deep’ as the correct term for this.
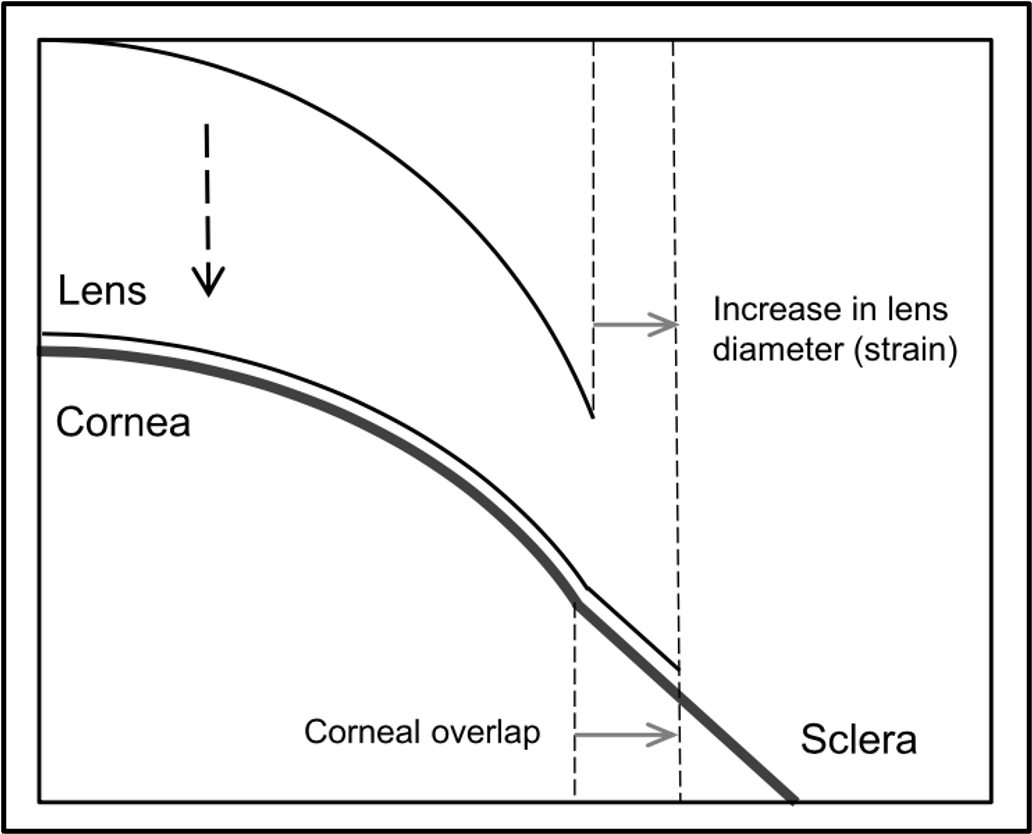
Indeed, Graeme Young already had published a paper in 2017 in Optometry & Vision Science showing that soft lenses by default increase in diameter when placed on the eye and need to do so, in fact, to achieve an acceptable lens fit. He coined the term ‘edge strain’, and an average edge strain of about 3% appears to result in a ‘good lens fit’. This means that given a constant temperature, a “good-fitting” 14.0 mm lens will increase to a 14.4 mm diameter when placed on the eye, or will have an on-eye diameter increase of 0.4 mm.
Ohio State studies
You might ask: How bad is it that a soft lens can be ‘good’, ‘deep’, or ‘very deep’ on the eye with no noticeable difference? These lenses most likely are all comfortable, at least in the beginning. But from clinical experience, we know that we don’t want a soft lens to be excessively deep, as this may lead to physiological problems including elevated redness and reduced underflow of fluid.
Indeed, a recently published paper by Matthew Andrew, Aaron Zimmerman and Melissa Bailey from The Ohio State University (US) showed that in eyes with more corneal infiltrative events (which are inflammatory markers), the lenses typically had a higher relative sagittal depth (meaning a deeper lens fit). In addition, at the American Academy of Optometry meeting last fall they presented a new study, including 57 habitual soft lens wearers showing that relative sagittal depth was significantly greater (a deeper lens fit) in participants who reported to have dry eye compared to those who did not report dry eye symptoms.
To put this in numbers, the relative sagittal depth was 360 microns for those who had no dry eye symptoms, while the groups who answered “unsure” or “yes” to the question about dry eye on the Contact Lens Dry Eye Questionnaire (CLDEQ) had relative sagittal depths of 540 and 500 microns, respectively: statistically significantly higher (p=0.008 for both groups). So, these findings suggest that higher relative sagittal depth values may play a role in soft contact lens dryness symptoms or lens wear comfort scores as well as in the development of corneal infiltrative events (inflammation).
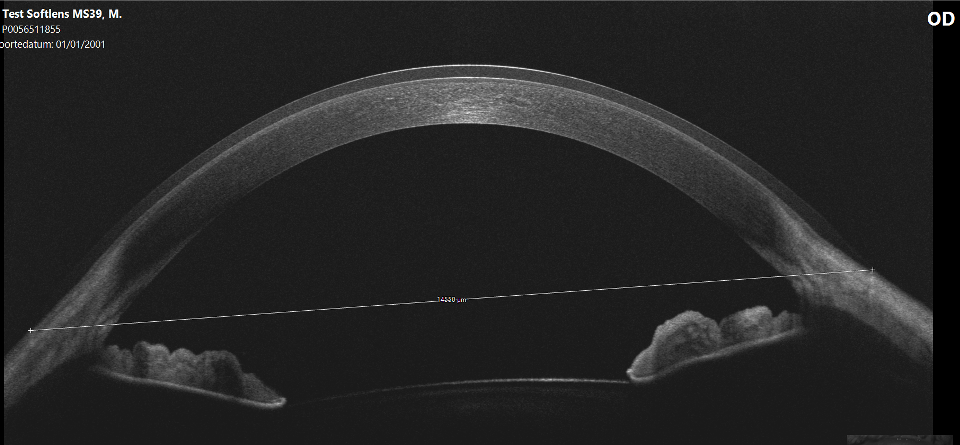
In the same studies, the researchers found a linear correlation between delta-SAG values (how deep the lens is compared to how deep the cornea is) and on-eye diameter increase. In short, optical coherence tomography (OCT) imaging showed that the deeper the lens, the greater the increase in diameter. This is an interesting finding that deserves more attention.
Pacific University project
As part of the ongoing soft lens fitting project at Pacific, we decided to replicate this study and to add another variable: a variety of base curves. Eight different lathe-cut lenses of known base curve and sagittal height (measured at eye-temperature, 34 °C) and a labelled diameter of 14.5 were manufactured by Mark’ennovy in Spain (Saphir, silicone hydrogel, Filcon 5B, 75% water content, Dk 60, modulus 0.13 MPa). They were placed on a standard (average) eye, and the on-eye diameter increase was measured using anterior segment OCT (Visante, Zeiss/Germany).
What is really intriguing is that the 7.7 mm base curve lens had an on-eye diameter increase of almost 1 mm (0.97 mm to be exact). One base curve flatter (8.0 mm) had an on-eye diameter increase of 0.77 mm; for the 8.3 mm base curve this was 0.53 mm, and for the 8.6 mm base curve a 0.27 mm increase was measured. For reference, the relative sagittal heights of these lenses were 680, 480, 248, and 46 microns (for the 7.7 mm, 8.0 mm, 8.3 mm, and 8.6 mm base curves, respectively).
Switching to flatter base curves of 8.9 mm, 9.2 mm, 9.5 mm, and 9.8 mm did not change anything; the diameter did not increase more than with the previous 8.6 mm base curve lens (the numbers were respectively 0.27 mm, 0.23 mm, 0.26 mm, and 0.23 mm increase). It’s important to note that the delta-SAGs of these four lenses were -143, -380, -520, and -650, respectively (note that these are negative values, so they varied from a little bit flatter to excessively flatter than the ocular surface).
The bottom line overall is that there was a steady decline in on-eye diameter gain from 7.7 mm to 8.3 mm base curves in roughly 0.20 mm steps for each base curve until a tipping point was reached at which the lens and ocular surface were on-par with each other, after which anything flatter no longer increased the on-eye diameter (the same increase in on-eye diameter was found compared to the previous lens base curve).
Finding DORYs
So, while in previous reports on soft lens fitting, we discussed ‘finding NEMOs’ (normal eyes measured ocular surfaces), the crucial thing now seems to be finding the optimal delta-SAG – or ‘Finding DORY’ to stay in the Disney theme, where DORY stands for ‘defined optimal reservoir yardage’, but then in microns. For the eye in our study, for instance, the optimal ‘DORY’ of these lathe-cut lenses was 248 microns. For normal eyes, this often could be the case. But the key point here is: to find the right lens, you need to measure the ocular surface of each individual.
Closure
To follow up on the latter, standard (disposable) lenses are great for the normal eye, and other variables such as material properties (modulus), surface treatments, lens design, and lens edge shape all play a major role in the success of lens wear (and dropout prevention). But it is at both ends of the spectrum of eye shapes that we can make a difference (and prevent these dropouts) – especially on the flatter end of the eye-shape spectrum, as we will see more ‘deep-fitting lenses’ if standard lenses are used for these eyes.
One thing that we need to make very clear in our practices, in our industry, and certainly in contact lens education at our institutions and our schools is that soft lenses should be fitted DEEPER on the ocular surface (for lathe-cut ánd for cast-moulded lenses), NOT flatter! Many schools still adhere to the basic and ancient rule (inherited from rigid corneal lens fitting) that soft lenses need to be fitted flatter (typically in the 0.6 mm to 1.0 mm range) than the central keratometry values. But that gives a completely wrong message to young eye care practitioners; soft lenses should not be fitted flatter than the ocular surface (a big myth indeed), but deeper. By how much, that is up for discussion and a potential subject for a future article in GlobalCONTACT. Some ‘grip’ is needed (a slightly deeper lens), as two recent papers from Spain indicate (Cruz-Crezpo et al. and Viñuela et al.).
Soft lenses are flexible and have a lot of leeway in this area, but anything less than 150 microns delta-SAG seems to be insufficient, leading to flat-fitting lenses with all the symptoms described earlier. Anything beyond 400 microns would be considered an excessive delta-SAG. Interestingly, this is the same as in scleral lenses. But these values could (and probably will) be different for cast-molded and lathe-cut manufactured lenses.
In summary: fitting soft lenses actually has much more in common with fitting scleral lenses (including using sagittal height values and creating an initial clearance before the lens flexes) than with rigid corneal lenses. It is important to reiterate that soft lenses are fitted deeper on the ocular surface, not flatter. This is an important distinction to make and an essential myth to debunk.
Read the article from Contact Lens Spectrum here
Eef van der Worp, BOptom, PhD, FAAO, FIACLE, FBCLA, FSLS is an educator and researcher. He received his optometry degree from the Hogeschool van Utrecht in the Netherlands (NL) and has served as a head of the contact lens department at the school for over eight years. He received his PhD from the University of Maastricht (NL) in 2008. He is a fellow of the AAO, IACLE, BCLA and the SLS. He is currently adjunct Professor at the University of Montreal University College of Optometry (CA) and adjunct assistant Professor at Pacific University College of Optometry (Oregon, USA). He lectures extensively worldwide and is a guest lecturer at a number of Universities in the US and Europe.
References:
Andrew M, Zimmerman AT, Bailey MD. The relationship between soft contact lens adverse events and corneal sagittal depth. Cont Lens Anterior Eye. 2025 Jul;48(4):102413.
Bailey, Zimmerman, Andrew. The Relationship between Soft Contact Lens Dryness Symptoms and Relative Sagittal Depth. Poster American Academy of Optometry. Boston (US). 2025
Cruz-Crespo JJ, Ortiz-Peregrina S, García-Gamero A, Rodríguez-Farfach F, Bolívar-Parra J, Ghinea R. Changing the paradigm of soft contact lens fitting: A sagittal height-based approach. Ophthalmic Physiol Opt. 2025 May;45(3):607-617.
Morgan et al. The International Contact Lens Prescribing Trends Consortium. Contact Lens Spectrum, January/February 2026.
Papas EB, Tilia D, Tomlinson D, Williams J, Chan E, Chan J, Golebiowski B. Consequences of wear interruption for discomfort with contact lenses. Optom Vis Sci. 2014 Jan;91(1):24-31.
Young G, Hall L, Sulley A, Osborn-Lorenz K, Wolffsohn JS. Inter-relationship of Soft Contact Lens Diameter, Base Curve Radius, and Fit. Optom Vis Sci. 2017 Apr;94(4):458-465.
Van der Worp, Lampa, Koijma. The Micron Wave. Contact Lens Spectrum, Sept 2025
Viñuela JR, Wolffsohn JS, Consejo A, van der Worp E, Piñero DP. Ocular surface characteristics and its association with soft contact lens fitting. Ophthalmic Physiol Opt. 2025 Nov;45(7):1715-1728.