The potential of scleral lenses

Large diameters can help when corneal lens fitting reaches its limits
Irregular corneal shapes have always posed particular challenges for contact lens fitters. Keratoconus, pellucid marginal corneal degeneration, postoperative scarring and corneal steps following penetrating keratoplasty or refractive surgery, as well as scarring following trauma, can significantly impair the optical quality of the corneal surface. While rigid gas permeable (RGP) lenses are traditionally considered the standard treatment, scleral lenses have established themselves in recent years as an important supplement and, in many cases, even as a superior treatment option.
Scleral lenses offer the possibility of creating an optically homogeneous, tear-filled boundary layer over the irregular cornea without exerting mechanical pressure on the central or peripheral corneal area. The sensitive areas of the cornea, which are highly innervated, do not come into contact with the lens when fully bridging scleral lenses are used, as the lens rests exclusively on the bulbar conjunctiva in the scleral area. This allows them to improve visual acuity, comfort, and long-term corneal health in situations where corneal lenses reach their limits.
This article provides a detailed overview of the advanced care options offered by scleral lenses for eyes with irregular corneas and systematically compares their properties with those of rigid corneal lenses.
Indications for scleral lens fitting
Keratoconus and other ectatic disorders
In keratoconus, the progressive bulging and thinning of the cornea leads to pronounced irregularity of the anterior surface. The irregularity of the anterior surface of the cornea is significant because it has a much greater optical impact than the posterior surface of the cornea, which borders the aqueous humor of the eye. While RGP corneal lenses can often be used successfully in the early stages, the tolerance of lens wearers decreases as ectasia progresses.
Typical fitting problems include inhomogeneous pressure distribution on the cornea, decentred lens fit and the resulting poor vision quality, as well as mechanical irritation.
In individual cases, these challenges can be exacerbated by very high eyelid tension (e.g. in neurodermatitis) and high refractive errors. Scleral lenses, on the other hand, completely bridge the conical area due to their design, which rests on the sclera, creating a stable, central tear chamber. This chamber-forming function reduces asymmetrical aberrations and thus improves optical quality.
Eyes after perforating corneal injuries
Scars formed after injuries are often irregular, asymmetrical, and difficult to describe topographically. Designing an appropriate contact lens back surface for these irregularities is a challenge. If additional factors such as high eyelid tension or high lens thickness due to a high refractive error that needs to be corrected are added to the mix, the fitting result may be suboptimal.
In such cases, corneal lenses can cause discomfort due to mechanical friction or become unstable. Scleral lenses avoid this problem as they rest on the sclera, which is usually regular in shape. Due to their minimal movement, they provide stable vision and are often considered very comfortable.
Condition after perforating keratoplasty (PKP)
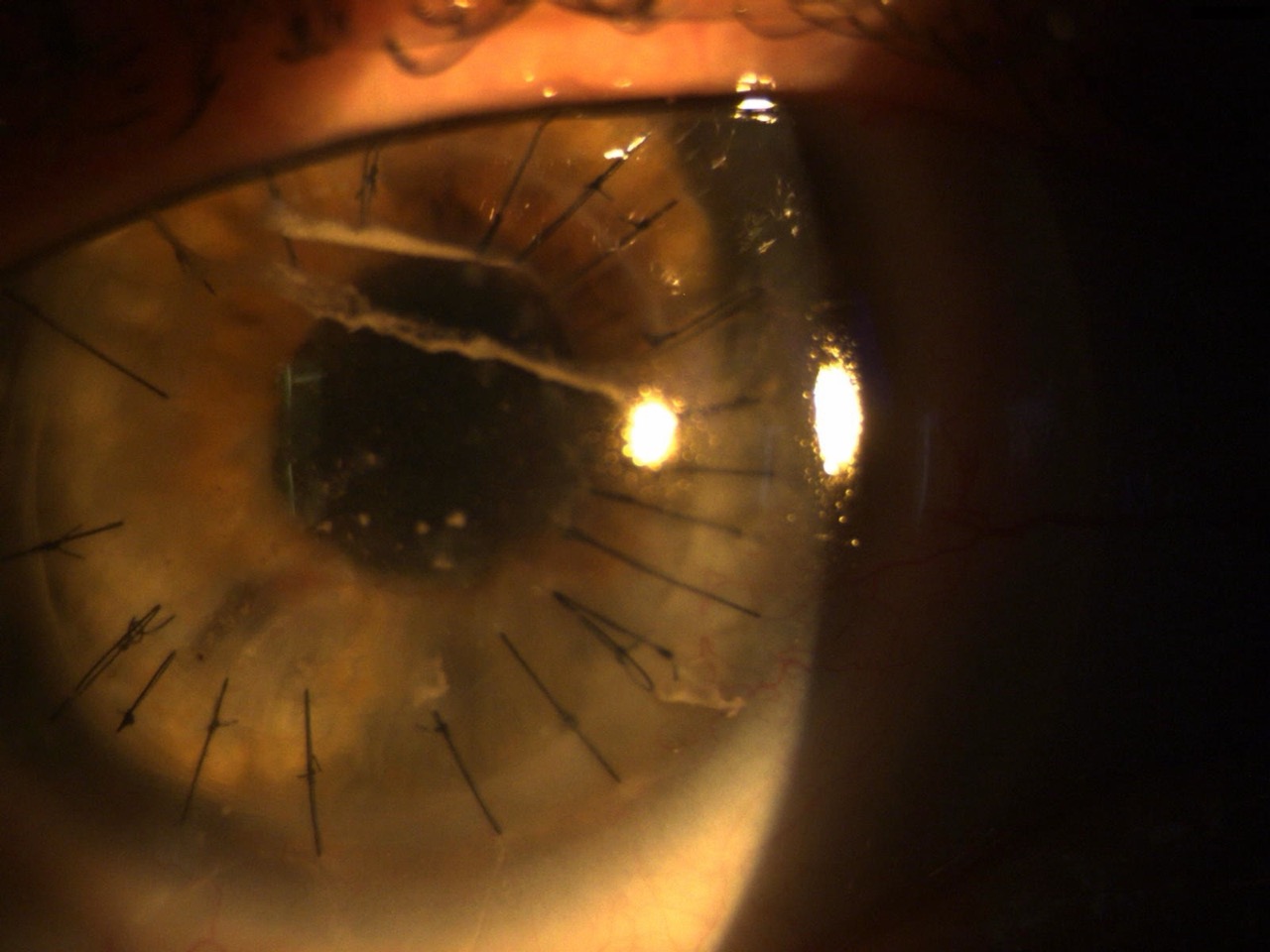
After corneal transplants, it is not uncommon for severe astigmatism or topographical irregularities to occur. Suture tension, graft size, and postoperative remodeling often lead to a complex height profile. Often, the preoperative prolonged cornea becomes an oblong cornea after surgery, which means it has flatter central radii and steeper peripheral radii. While RGP corneal lenses can be perfectly functional for PKP patients, practitioners often face challenges such as pressure near the transplant, microerosions, or contact lens decentration. Scleral lenses can be used to bridge the irregular cornea (vault) and achieve a uniform vault structure over the transplant. This not only reduces mechanical stress to a minimum, but also creates an optically customizable zone.
Dry eye disease (DED) and ocular surface disease (OSD)
Scleral lenses have also established themselves as an important therapeutic option for severe or treatment-resistant forms of dry eye and other diseases of the ocular surface (e.g., Sjögren’s syndrome, GvHD, Stevens-Johnson syndrome, persistent and recurrent epithelial defects). The post-lenticular fluid chamber ensures constant moisturization of the cornea, prevents evaporation, and protects the corneal surface from mechanical friction caused by the eyelids. Therefore, scleral lenses are recommended in current management algorithms (e.g., TFOS DEWS III1) as an option for more complex cases. Similarly, the relevant literature reports on treatments following eyelid injuries in which scleral lenses were able to prevent the drying out of the eye surface2.
Optical objective: production of an optically flawless surface
The optical principle of scleral lenses is to replace the irregular front surface of the cornea with a regularly shaped lens surface, separated by a tear reservoir that acts as an optically homogeneous intermediate medium. The optical improvement is based on three points:
- Neutralization of irregularities
The tear fluid completely fills in any unevenness and acts like a refractively homogeneous film. - Minimization of higher order aberrations (HOAs)
The reduction of asymmetric aberrations, namely coma, is clinically significant and has been documented in studies. - Constant refractive conditions thanks to stable fit
Since the lens sits on a large area of the sclera, scleral lenses show significantly less movement than corneal lenses and are therefore superior in terms of visual stability.

Fitting scleral lenses
When considering the fitting of scleral lenses, the author recommends the use of trial lenses for several reasons. On the one hand, this allows the basic tolerance of scleral lenses to be determined quickly and efficiently. In addition, it is easy to assess the fit, the thickness and shape of the tear film, the over-refraction with measurement of the achievable final visual acuity, and to determine the final prescription lens parameters. The corneal diameter, the shape of the cornea (prolonged or oblong), and the required vertex depth of the measuring lens, which is necessary for a fully bridging lens fit, are decisive factors in the selection of the first trial lens. When the anterior segment of the eye is measured using Scheimpflug technology or profilometry, information about the curvature and regularity of the sclera can often be taken into account at the same time.
The chamber-forming effect of scleral contact lenses fills corneal irregularities in the optical path with a homogeneous, tear-like fluid. This reduces higher-order aberrations (HOA), and in particular asymmetric aberrations such as coma. Prospective comparisons show significantly lower total aberrations (total HOA), coma, and trefoil under scleral lenses compared to RGP corneal lenses (e.g., Knoeri et al.)3. Some reviews report improvements in visual acuity and night vision. These findings explain the frequently observed, clinically relevant improvement in visual acuity in patients with keratoconus, post-transplant irregularities, or scarred corneal changes.
Biomechanical differences: sclera and conjunctiva instead of cornea as contact surface
Rigid corneal lenses
Corneal lenses ideally position themselves on the tear film in front of the cornea with sufficient pupil coverage. The fit is assessed in terms of surface fit by observing the tear film stained with a sodium fluorescein solution. The main variable here is the tear film thickness, which can fluctuate with increased tear secretion after insertion of the corneal lens. In cases of regular or only slightly irregular corneas, varying tear thicknesses under the contact lens do not pose any biomechanical problems. However, in cases of severely irregular corneas, there are risks ranging from pressure points over cone tips and epithelial compression to corneal damage. If hard apical or paracentral contact points occur during corneal lens fitting in cases of irregular corneal conditions, the localized mechanical stress on the cornea can become so high that it results in stainable areas with spots or even deep corneal lesions.
When assessing the fit of scleral lenses, sodium fluorescein solution is used to estimate corneal bridging using a slit lamp. To do this, the narrow slit can be observed at a 45° angle and the thickness of the fluorescein layer can be compared to other known measurements, such as lens thickness.
Since scleral lenses rest exclusively on the bulbar conjunctiva in the scleral area, it is important to note when assessing fit that the estimated or measured corneal curvature is highest after initial insertion and decreases with prolonged wear due to compression of the bulbar conjunctiva. A good starting value for central corneal bridging is between 250 and 350 µm.
Scleral lenses
Scleral lenses completely cover the cornea and rest exclusively on the consistent, less sensitive sclera. Advantages include:
- No mechanical stress on the cornea
- Significant increase in comfort
- Stable position even with extreme irregularity
- High optical repeatability because the position hardly varies
This biomechanical decoupling is one of the main reasons why scleral lenses are increasingly preferred for the treatment of irregular corneas.
Comparison of corneal lenses and scleral lenses in everyday clinical practice
Fittability and reproducibility
Corneal lenses require very precise fitting to the corneal contour; in cases of irregular corneas, several trial lenses are often necessary. Scleral lenses, on the other hand, automatically compensate for many irregularities using the vault technique; modern OCT-assisted procedures significantly increase efficiency.4
Visual acuity and optical quality
Both systems achieve good results with moderate irregularities; however, in cases of severely irregular corneas, scleral lenses demonstrate a superior reduction in HOAs in numerous series and thus often yield better visual acuity and night vision results.
Wearing comfort
RGP corneal lenses can cause a foreign body sensation due to eyelid interaction. Scleral lenses often offer a more comfortable and stable fit, which improves compliance.
Oxygen supply
RGP corneal lenses generally offer good oxygen transmission, supported by the tear pump. Scleral lenses prevent direct tear circulation; this requires the use of highly gas-permeable materials (high DK) and optimization of the central chamber thickness to minimize hypoxic risks. Modern materials and careful fitting significantly reduce these risks.
Technological advances: The key to the importance of scleral lenses today
The renaissance of scleral lenses can be attributed to technological developments:
- OCT-assisted vault analysis for precise fittings.
- Individual peripheral zone designs (toric, quadrant-adapted) for better scleral alignment.
- High-DK materials for long daily wear times.
These advances now enable highly customized care that combines optical performance and physiological compatibility.
Limitations and challenges of scleral lens fitting
Despite their advantages, challenges remain:
- Increased hygiene and handling requirements (filling technique, cleaning).
- Risk of hypoxic changes with suboptimal fitting or unsuitable materials.
- More complex aftercare (controlled vault follow-ups, monitoring of scleral contact).
- The cost of customized lenses is higher than that of standard RGP lenses.
In DED/OSD patients, specific problems such as midday fogging, poor lens wettability, and handling limitations must also be taken into account; these should be addressed during the consultation and follow-up care.
Practical recommendations for contact lens fitters
- Carefully check the indication:
Keratoconus stage ≥ II–III, post-PKP irregularities, scarred corneal defects, persistent DED are classic indications. - OCT-assisted initial fitting:
Measure corneal topography and determine the desired central vault height (clinical target values depending on laboratory/design). - Material selection:
Prefer high DK materials (where possible >100–150); keep lens thickness and vault minimal, but clinically adequate. - Follow-up care:
Repeated OCT checks at the latest one, two, and four weeks after insertion; more frequent checks of the epithelial status in DED patients. - Patient education:
Filling technique, hygiene, handling, warning signs (redness, pain, deterioration of vision) — and clear agreements on follow-up care.
Conclusion
Scleral lenses are now an indispensable tool in the treatment of irregular corneas. By creating a tear-filled reservoir over the cornea, they have been proven to reduce higher-order aberrations — namely coma — and in many cases improve visual acuity and subjective visual quality. Scleral lenses are often the better (and frequently the only) non-surgical treatment option, especially in advanced forms of keratoconus, after corneal transplants, in cases of scarring, and in therapy-resistant forms of dry eye. Rigid corneal lenses remain valuable in early/moderate stages, but are increasingly supplemented or replaced by scleral lenses in cases of pronounced irregularities. Modern OCT technology, customized designs, and improved materials have significantly increased the safety and effectiveness of scleral lenses.
Stefan Schwarz, Dipl.-Ing. (FH), FAAO, MCOptom, and Diplomate in Cornea, Contact Lenses, and Refractive Technologies at the American Academy of Optometry. He is a renowned expert in contact lens optics and ocular physiology. Thanks to his national and international lecturing activities, research contributions, and many years of practical experience in his own practice, he is one of the recognized experts in modern optometry.
References:
- Jones L, Craig JP, Markoulli M, Karpecki P, Akpek EK, Basu S, Bitton E, Chen W, Dhaliwal DK, Dogru M, Gomes JAP, Koehler M, Mehta JS, Perez VL, Stapleton F, Sullivan DA, Tauber J, Tong L, Travé-Huarte S, Wolffsohn JS; TFOS Collaborator Group. TFOS DEWS III: Management and Therapy. Am J Ophthalmol. 2025 Nov;279:289-386. doi: 10.1016/j.ajo.2025.05.039. Epub 2025 Jun 2. PMID: 40467022.
- Chaudhary S, Chatterjee S, Jain N, Basu S. Scleral contact lenses for optimal visual recovery in a case of severe acid burn with total lagophthalmos. BMJ Case Rep. 2022 Jul 5;15(7):e248384. doi: 10.1136/bcr-2021-248384. PMID: 35790322; PMCID: PMC9258505.
- Knoeri J, Mhenni R, Friquet C, et al. Comparison of optical aberrations in keratoconus with scleral versus rigid gas permeable lenses. Eur J Ophthalmol. 2024 Mar;34(2):394–398. doi:10.1177/11206721231221588. PubMed PMID: 38128913.
- Barone V, Petrini D, Nunziata S, Surico PL, Scarani C, Offi F, et al. Impact of Scleral Lenses on Visual Acuity and Ocular Aberrations in Corneal Ectasia: A Comprehensive Review. J Pers Med. 2024;14:1051. doi:10.3390/jpm14101051.